Wednesday, April 30, 2014
Stats and Reflection
Our BOINC GPU grid computed 131 units for the Barcelona Biomedical Research Park - Molecular Simulation of Proteins. This means that through the duration of this project, our computer looked at 131 units of proteins using its computational power. 19,111 tasks are currently in progress on this grid, and we have contributed to one of them. This company currently has 45,000 computers computing for this research. It really shows how much power is needed to do these simulations for their research. We find this incredible because we feel like we helped make a difference without really doing direct work. It's crazy how technology is advanced enough that we were able to contribute to research. It's amazing how anyone in the world with an electronic device with computational power can help contribute to any research that they are interested in by simply downloading a program. This project really helped bridge the gap between the concepts we were learning in class to real world research and issues. We were able to make new connections between a commonly known disease to evolutionary ideas we learned. We would have never taken this approach in looking at Schizophrenia. If it weren't for this project, we wouldn't know about the power of grid mapping and using blogs.
Wednesday, April 2, 2014
Schizophrenia Q&A
Questions – Schizophrenia
These questions address the Schizophrenia Bulletin article entitled “Schizophrenia, Psychiatric
Genetics, and Darwinian Psychiatry: An Evolutionary Framework” by Peralson and
Folley, 2008.
- Is
schizophrenia a qualitative or quantitative trait? What is the estimated heritability of
this phenotype?
This is most likely a multi-gene
trait with common alleles that are risks to causing this disease. By themselves, those genes would not cause
the disease, but when they all come together the disease is manifested
(polygenic disease). All genes are
needed for the disorder to be present.
This makes it a quantitative trait.
No specific genes are linked to Schizophrenia, but a number of genes
contribute to causing the disorder. They
increase the probability of the disease manifesting in a person.
In
concordance studies with twins, in identical twins, they are forty to sixty
percent likely to get the disease, as opposed to fraternal twins that are ten
to twenty percent likely to get the disease.
This indicates that genetics has a lot to do with the cause of the
disease, but environment still plays a point (“The Heritability of
Schizophrenia”). Disequilibrium studies
have also been performed. In these
studies, large families affected by the disease are studied and their
chromosomes are compared to families who are not affected. From these studies, it has been shown that no
specific chromosomal locations have been found that specifically cause the
disease. A variety of loci contribute to
causing the disease. When assessing
families with Schizophrenia, the family genes are combined for assessment
because of the smaller family size. This
can cause issues to identifying specific genes that cause the disorder because
some families may have different genes specifically causing the disease than
another family (“Schizophrenia and Genetics”).
- What
kind of inheritance explains the observed patterns seen in schizophrenia?
It is the unfavorable combination
of specific genes that contribute to neuron and brain development. These changes in the genes are due to copy
number variance and single nucleotide polymorphisms within the normal
range (refer back to question 1 for more specifics).
- Why
do schizophrenia risk genes persist in evolution?
The genes themselves are not
selected against when inherited singly.
They are “below the radar” of selection.
Some inherited individually have a compensatory advantage or are neutral,
keeping them in the population. These
genes are only selected against when the right combination is inherited and the
disease occurs.
- What
are the possible heterozygote advantages associated with schizophrenia? Do you agree?
These alleles alone can be
associated with normal or increased fertility, making them advantageous. Another advantage associated with Schizophrenia
for the genes would be in an ancestral environment. An example of how these genes came to be
would be through “broken genes”. For
example, some genes provided protective advantage with salt retention when salt
was not readily available in the environment.
Overtime, keeping this trait when sodium is now plentiful contributes to
the elevated levels of hypertension seen in society today. There is a similar idea with diabetes. In the ancestral environment, these genes
expressed hormones that caused insulin resistance that helped with more
effective fat storage, helping with limited availability of food. Now this trait is disadvantageous and causes
elevated levels of obesity in people with this disease because of unnecessary
fat storage. These genes are associated
with causing diabetes. There might have
been adaptations that Schizophrenia susceptibility genes caused, but they have
yet to be identified. Schizophrenia
might have been advantageous in causing paranoia in ancestral environments,
helping protect the person from predators or other possible dangers. We agree with these ideas the paper
presents. As the environment changed
over time, the advantages the genes offered also changed. Because of modern medicine, these traits will
be retained in the population, as these issues most likely can be treated. Also, carriers will continue to contribute
these traits to the next generation.
- If
heterosis is acting on the schizophrenia alleles, what might you expect
will happen to these alleles over the long term ? (Think fitness tables...)
If heterosis is acting on the
schizophrenia alleles, you would expect that over a long period of time the
heterozygote genotype will become fixed in the population with the homozygote
dominate and homozygote recessive genotypes going to an equilibrium based on
the frequency they are at during the time heterosis is selected for. This means that the schizophrenia alleles
will always be in the population. There
will always be a small population of people who are affected by schizophrenia
because currently only one percent of people are affected.
- This
paper, and much of evolutionary psychology, is panselectionist or
ultradarwinist. What does that
mean? What other mechanisms of
evolution might be at play here?
A panselectionism is the belief
that the only mechanism of evolution was natural selection and that all genes
are inherited (“Neo-Darwinism”). An
ultra-darwinist is a person who believes in Darwin’s idea of natural selection,
but thinks that it is the only mechanism of evolution (Cain 220). This paper emphasizes these ideas greatly,
putting great consideration on natural selection in the evolution of the
schizophrenia genes. The paper briefly
mentions that sexual selection may have caused schizophrenia to appear in the
population. Exaptation is also
mentioned, as some of these genes may have started being used for other
functions like speech and art. Other
mechanisms of evolution that should be considered when analyzing these traits
should be mutations, genetic drift, and gene flow. There might have been disadvantageous
mutations that caused these alleles to become present in the population. Founder affect might have occurred, bringing
together a population with these alleles that would increase the frequency of
inheriting schizophrenia susceptibility genes.
Gene flow might have then integrated these alleles into larger
populations over time.
If you want to read more, check out this link: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2632450/
Works Cited
Cain, Clifford Chalmers. "Darwin's Pious Idea: Why
The Ultra-Darwinists And Creationists Both Get It Wrong - By Conor
Cunningham." Reviews In Religion & Theology 19.2 (2012): 220-221.
Academic Search Complete. Web. 2 Apr. 2014.
"The Heritability of Schizophrenia." Biological
Basis of Mental Health. Open Educational Resources, n.d. Web. 2 Apr. 2014.
"Neo-Darwinism." Princeton University.
N.p., n.d. Web. 02 Apr. 2014. <http://www.princeton.edu/~achaney/tmve/wiki100k/docs/Neo-Darwinism.html>.
"Schizophrenia and Genetics: Research Update | Psych
Central." Psych Central.com. N.p., n.d. Web. 02 Apr. 2014.
<http://psychcentral.com/lib/schizophrenia-and-genetics-research-update/0008736>.
Wednesday, February 12, 2014
Specialist Interview
Specialist Interview
Started at 4:00 PM 2/12/14
Started at 4:00 PM 2/12/14
For our interview, we chose to talk to Dr. Saz Madison from the Psychology Department at Rockhurst University. Here are the notes from the interview:
1.
What is your attitude on dealing with patients
affected by schizophrenia? Do you enjoy
working with them?
Saz: I have. Very much… Any population I work with, I consider
the situation a person that is dealing with (x) whatever the psychological
dysfunction. This is an individual. I do
what I can to understand and predict and intervene in regards to their
lifestyle. When I see a schizophrenic,
mostly I experience determination and excitement. I enjoy working with populations who
experience significant psychological disabilities. People think of it as a diagnosis. It’s really more accurate to recognize that schizophrenia
as a constellation of disorders. Many different
subtypes constitute to a set of disorders.
It’s hard to say how I like working with it.
Sarah: cuz it varies
so much
Saz: right. For example catatonic – muscular not as
active
Paranoid schizophrenics are more active because they experience
hallucinations. It might be exhausting dealing with emotionally effusive schizophrenics
with a flattening affect because there are intense types of interactions.
2.
As a psychologist, how are schizophrenics’
brains different from a normal person’s brain?
·
There is less grey matter in a schizophrenic’s
brain. Fluid filled area (think central ventricles)
they are larger in a person with schizophrenia evidence of tissue
atrophy/loss. In terms of overall brain
tissue there tends to be less.
·
Increased activity in dopamine pathogens and
might be responsible for positive symptoms of schizophrenia. We don’t know if we get these changes in
neuro-anatomy or neurophysiology as a result of the onset of the disorder or if
these changes are from development of disorder.
·
Consistently evidence of tissue loss or atrophy
from the onset of this disorder. We don’t
have a lot of very definitive evidence for this. There is evidence for decreased activity in
the limbic system changes in function of the hypothalamus, not any particular
structures, some changes in function of the thalamus (which makes sense if
thought responsible for interpreting info about senses and then we have
hallucinations that are sensory in nature).
·
When some schizophrenics have speech problems
then they may have differences in their Brocca’s and Wernicke’s, the primary
language areas of brain. If we don’t use
parts of our brains then different areas of the brain encroach on that area of
brain.
·
Don’t know if changes are from thought
disorder/language disorder resulting in neurological changes. Neurological anomalies result in the
development of the disorder.
3.
What challenges are associated with treating
patients affected by schizophrenia?
·
Saz:
answer on two levels. Challenges overall
and challenges with specific patients
·
Typically poor treatments for some aspects of schizophrenia. Positive symptoms of
schizophrenia have pharmacological treatments, whereas negative symptoms are
difficult to treat. Positive symptoms are
things you get during onset, negative are things you lose, like emotional
mobility.
o
Example of student: so excited to see student haven’t seen in a
while then realize they’re going to prison oh no!
o
Males are more likely to experience negative
symptoms
·
Professionals are not good at treating emotional
issues. Much better treatments for,
getting a little better at treating emotional reciprocity…
·
positive treatments have great treatments (drug
treatments) antipsychotics. Do a good
job with positive symptoms. Hallucinations
and delusions. Good at doing that
·
Challenges in general are trying to figure out
ways to intervene with negative symptoms in schizophrenia.
o
Specific patient: youngest schizophrenic/person he felt was
appropriately diagnosed was 17 years old and one of his negative symptoms was
he had severe atonality (like when we talk our tone changes, might go to
something different, helps communicate with things).
o
Had serious affecting flattening – tonal completely
delayed experienced emotions when talking (monotone). Once lived in an inpatient facility and we
were taking them and some of the other residents on a day trip a canoe
trip. He was afraid of water. So on the trip, he’s in a canoe with me and
we’re going and he’s just sort of sitting there and I said you seem very very
quiet and he goes (shakes head) and that’s it and well that’s ok and we keep
talking and these are the things we’re going to try.
o
The river had many turns and a branch touched
his face and he says oh no oh no oh no and he flips the canoe and ends up in
the water and he’s just so afraid and he’s terrified and says can’t swim can’t
swim and while I’m getting my arm around him he couldn’t communicate to me the
fear he was experiencing.
o
Normally, when he got angry his voice would get
a little louder.
o
Couldn’t scream when he fell in water just
loudly spoke.
o
Got to the side of the river and on shore and he’s
expressing the same emotions tonally except tears are going down his face. How could I have anticipated that this would
have happened in this experience? Earlier
when I was enthusing about the canoe trip, was he trying to communicate to me
what he felt? It’s challenging in
regards to how do I get to the point where I’m good at anticipating that this
individual will respond (how they will respond and what’s the best way to
respond to them)
4.
There are several subtypes of
schizophrenia. Is there a subtype that
you’ve experienced more than others?
·
Paranoid schizophrenia – it’s so significantly
more common than the others that probably unless someone is specialized in a
particular type it’ll be paranoid with positive symptoms
·
hallucinations and/or delusions (more
frequently)
o
Hallucinations are still very very frequent in
paranoid schizophrenia. In terms of
symptom prevalence paranoid with delusions of persecution. ßanecdotal
– probably the most common delusions found in people with paranoid schizophrenia. Any delusions, false belief that there are
forces outside of myself that are allied against me in some way.
o
Example: It
may be in the form of I’m a university professor and I feel like my students
are working against me so I won’t get hired and that one student is a super
hero who is using her power to influence others to get students to get at me
and I know this because I have had encounters with aliens before. If I don’t engage in some behavior designed
to protect me from then then I’ll be vulnerable.
·
Sarah: How
do you deal with those interactions (without laughing)?
·
We laugh but the fact of the matter is any time
we go into any field before we get into it and learn about it (especially
post-grad education), we often think that we know how we will respond in
certain situations. We mature in knowledge,
understanding, and professionally. I was
absolutely sure when I went to Rockhurst that I wanted to be a child
psychologist. Ended up that I didn’t
have the emotional maturity to deal with it.
Swore would never do it again. In
undergrad I was not aware enough of what I would want and experience. When experienced in grad school, I was not
emotionally or intellectually prepared for the encounters in childhood
psychology. Now I can work with any
population and I can respond to it.
o
Purpose of rotations in grad school – really all
part of professional development (literally us developing into a
professional).
1.
What are some of the most common misconceptions
about the disease?
o
First one thinks of bothers him a lot. People see them as
dangerous/threatening. A good way to
characterize it is you picture the person standing on street corner talking to themself. Oh hey there’s that crazy person. Parent with children pull kids closer. In actuality them engaging in negative acts is
very unlikely, even more unlikely compared to normal people.
o
We presume that because they suffer from
psychological dysfunction that they are dangerous. Significant mistreatment of them. Leads to isolation. We could avoid this. They could have a better quality of
life.
o
Major misconception: relates to what we talked about. Schizophrenia means one thing that it’s one
disorder which we can list criteria for.
However, it is a constellation of disorders. Believe it could better be thought of as a
schizophrenia spectrum disorder. Much like
autism spectrum disorder considered now.
The way it manifests itself in regards to the different types, they are
all so fairly distinct but also functionally different. We can anticipate different symptoms, levels
of functioning, ability to engage in activities of daily living (for example)
depending on the type.
2.
Are there are any alternative treatments for the
treatment of this disease? Do you think
they’re effective?
o
For positive symptoms I said psychopharmacology
for positive symptoms best treatments
o
Talk therapies have yet to show empirical data
o
Cognitive therapies remediate some of the
negative symptoms
o
Ex: we
talked about lack of social reciprocities:
behavioral social skills training interventions actually train the person
with the disease who is experiencing symptoms
o
They can be taught to respond appropriately by
helping them recognize social behaviors ex:
how to respond during a funeral or when to laugh and when not to
o
interventions are designed to increase my
ability to engage in daily activities and get out and maintain employment,
healthy relationships, romantic interpersonal relationships. Behavioral interventions (most empirical
support)
MISCONCEPTION: can I say
one thing about a misconception
o
A major misconception is that people think it’s
a split personality. That’s a completely
different disorder (dissociative identity disorder). Because it is schizophrenia and that it
translates as “split mind”, they think that it means split personality. Example:
Jim Carry movie – me, myself, and Irene – media feeding misconception
Have you ever heard about Jeni? How do you feel about her?
o
Childhood diagnosis of major psychological
disorders is bad. Earlier this year, not
me being/distracting, the APA released latest DSM5: where we define what schizophrenia is. One of the trends in DSM5 does a greater deal
with childhood manifestations
o
The average age of onset for schizophrenia
positive symptoms is young adulthood – very late teens into twenties this is
when it typically manifests itself.
o
Anything pre-pubescent aka any time diagnosis is
made pre-puberty, I tend to be skeptical about those diagnoses. There might be a better explanation for the
behaviors being seen. I am very behavioral
oriented. I believe that behavioral
theory could go a long way in explaining the presence of many of these
behaviors that are associated with schizophrenia in children.
o
Example: Have
an obsession with set of items and engage in obsessive relationship with them (ex: believe media is talking to them). Behavioral theory suggests that those
behaviors are shaped by the reinforcement in their environment and maintained
by the presence of their environment.
o
Example: If
you give attention for a behavior – child is being reinforced for performing
behaviors (parents or teachers expect them to act that way, provide
reinforcement for when they do behavior).
o
Example:
child who throws temper tantrum – parents – fix kid. My first thought is why are you paying them
to throw temper tantrums. How do you
respond when they do it? You respond the
way they want (too busy to pay attention).
o
Example: Friend
is over, child throws temper tantrum for sweets, you’re embarrassed so you give
them a cookie. Child got what he/she wants,
which increases likelihood of behavior
o
Behavioral theory can explain some adult
schizophrenics. Look at other possibilities
before you think it is actual childhood onset.
Is it possible? Yes, literature
says that it is. Have I ever seen a
child be diagnosed with it? No. Youngest experience = seventeen year old with
schizophrenia – agreed with diagnosis, a little skeptic at first but eventually
agreed
o
Should look for alternative ideas for treatment
o
Our field (parent fields: philosophy and biology) this sort of
biological model, medical model that a lot of clinicians employed really leads
us to look for a diagnosis which often leads us to missing the individual. Might miss things that are specific to the
individual. Might be environmental
conditions from parents behaviors – symptoms may be from psychosocial or
environmental
o
Monica:
parents just want a label, don’t really care what’s going on just want
to label kid
o
Saz: look
at it from parent or sibling, boy doesn’t it feel so much more comfortable to
know what it is. For professionals, to
understand and intervene, we don’t have that luxury or at least it’s not
appropriate for us. It’s lazy and
unethical. I think it’s important that we
look at the individual that is experiencing these things and respond to that
individual. If you get a diagnosis, that’s
great for communication and treatment planning, but the important thing is the
individual and they are idiosyncratic.
Sadly, we use this sort of population/data driven approach to make a
decision about an individual sitting in front of us. Want to respond to that individual first…
sometimes there’s an over reliance on diagnosis
o
Think of it as people experiencing these life
challenges – may be better to describe by explaining with this disorder or this
disorder. We are trying to understand
human beings (don’t rely on label)
o
Danger to paying more attention to a diagnosis overall
as opposed to the individual. When looking
at a diagnosis and no longer the person, you may miss something
o
Respond on level of individual not the level of
the diagnosis. Look at the whole picture
not just one little side.
1.
What kind of perspective should people take?
o
Saz: the
way he approaches them, working with them, they are people who are suffering
from psychological distress problems in life.
The way that we approach interacting with them initially family member,
clinician is as that they are another human being. They have had experiences that we cannot
understand. These people who are
experiencing these difficulties that we cannot understand may be experiencing
life differently because of misconceptions due to their disease. They are treated poorly and they almost
anticipate being treated dismissively or badly. It’s a really unfortunate thing.
o
Approach them:
I like this part of the question.
Need to remember that schizophrenics recognize that they see the world
differently and inaccurately. It’s not
consistent with the reality that everyone else experiences. Now imagine coming to understand that the way
you understand the world is not like anybody else. All of these things I believe are wrong. Someone who has visual or auditory
hallucinations: I have this friend I see
all the time… what? what do you mean
they do not exist. This is the reason
depression is so frequent with diagnosis of schizophrenia.
o
We should approach them with compassion and try
to be as understanding as possible. We have
to approach them with humility. If we go
into interactions and expect what they’ll be like, we go in with assumptions
that will mislead us with the interaction.
Interview ended at 5:04 PM 2/12/2014
Reflection:
1.
It was very insightful. I learned things I had never thought of
before. Dr. Madison told many good
stories. We really enjoyed his quote
that we are trying to understand human beings not focusing just on
diagnosis. I learned how schizophrenics
saw the world and how diverse the disease is.
When we asked him about misconceptions, he opened our eyes to many
different aspects of this disease.
2.
From the interview, we had a change of
insight. We feel more caring and
compassionate toward schizophrenics. We
feel less afraid of approaching people with this disease. Dr. Madison told us to approach
schizophrenics with compassion and humility.
3.
The only thing that disturbed us from the
interview was his example of his patient that could not express his
emotion. We felt that it would be
frustrating as the therapist to have to find ways to understand and help with
that. We were also disturbed by the one
size fits all diagnosis that is given by many psychologists that help people
with psychological disorders.
4.
The connections we had between the interview and
the classwork we have been doing was how he mentioned that schizophrenia can be
highly hereditary. Also, we had asked
him about how schizophrenia affected brain function in an attempt to compare
what he said to what we had researched in our first blog post. Dr. Madison also seemed very surprised and
interested in us contributing to grid-computing for our evolution class.
Wednesday, January 22, 2014
Introduction to the Project
What Is Schizophrenia?
Schizophrenia can be defined as a severe brain disorder
in which its victims abnormally interpret reality. People with schizophrenia
show symptoms of hallucinations, delusions, thought disorders represented by
uncommon thought processes, and movement disorders where patients express
frantic body movements. Schizophrenics also suffer from disrupted emotions and
behaviors that lead the patient to be dissatisfied with everyday life and lack
the ability to endure planned activities. People with schizophrenia often speak
without making sense and may sit for extended periods of time without moving.
They also express cognitive symptoms such as experiencing difficulty
understanding information and paying attention and suffer from memory problems.
Therefore, Schizophrenics have difficulty holding jobs and caring for
themselves.
Schizophrenia occurs around the world and affects men and
women equally. The disease occurs in all ethnic groups at comparable rates.
Symptoms commonly arise between the ages of 16 and 30. Schizophrenia rarely
occurs in children and usually does not occur in people over the age of 45.
Schizophrenia may be difficult to detect in teenagers due to early
schizophrenia symptoms, such as irritability, trouble sleeping, a decline in
school performance, and feelings of withdrawal from friends and family, being
common in this age group. Additionally, men often experience symptoms earlier
in life than women.
The causes of schizophrenia are not known. However
research has led to conclusions of schizophrenia being influenced by genetics
and environmental factors. Complications with chemicals in the brain and
neurotransmitters, dopamine and glutamate, may contribute to the development of
schizophrenia. Studies involving neuroimaging compare the brain structure and
central nervous system of people affected with schizophrenia to those not
affected. The comparisons lead schizophrenia to be thought of as a brain
disease. With this, people diagnosed
with schizophrenia have differences in their brains. Some differences are the
larger fluid-filled cavities in the center of the brain, less gray matter, and
some areas of the brain experiencing more, or sometimes less, brain activity.
Moreover, Schizophrenia has been known to run in
families. Chances of developing the disorder are higher in people who have
first-degree relatives with schizophrenia. Using this, scientists consider
several genes to be linked with a higher risk of developing schizophrenia, with
no single gene causing the disease in its own. Research has found that people
with the disease have higher rates of genetic mutations, which concern hundreds
of genes that may disrupt brain development.
According to the National Institutes of Health, studies propose that
schizophrenia may result when a gene that is imperative to making brain
chemicals errors. Scientists also believe that schizophrenia may develop when
there are certain interactions between genes and the environment. Environmental
factors such as the introduction of viruses, malnutrition before birth, and
problems during birth may contribute to the development of schizophrenia later
in life.
Today, it is still unknown what causes schizophrenia.
From that, doctors have to treat symptoms instead of the root problem. To
do so, doctors prescribe antipsychotic medicines such as chlorpromazine,
haloperidol, perphenazine, and fluphenazine. These medicines are older,
so doctors refer to them as typical antipsychotics. More recently
developed antipsychotics are referred to as atypical, and examples of these are
risperidone, olanzapine, quetiapine, ziprasidone, aripiprazole, and
paliperidone. With all medications, there is a possibility for side
effects. With these antipsychotics, possible side effects are dizziness,
drowsiness, blurred vision, rapid heartbeat, skin rashes, sensitivity to
sunlight, and menstrual problems for women. Atypical antipsychotic
medications can cause additional problems, including weight gain and metabolic
changes. These side effects can lead to an increased chance of the
development of diabetes and high cholesterol. Typical antipsychotics also
have specific side effects. These antipsychotics can cause problems with
physical movement, such as muscle spasms, rigidity, restlessness, and
tremors. Long term use of these typical antipsychotics can cause tardive
dyskinesia, which is a condition where a person makes movements they cannot
control. This condition usually affects muscles around the mouth.
Psychosocial treatment can also be utilized to
help patients cope with every day challenges due to their illness (every day
care, work, communication, etc.). Family education can also be helpful in
treating a patient. By working with therapists, families can find ways to
develop good coping and problem solving skills for the family and their
affected loved one. Cognitive behavioral therapy can also be used to help
patients learn to cope with symptoms of their disease that do not go away with
the use of their medications. Self-help groups can also be good for those
with schizophrenia as it gives them another support group to help them feel
like they are not alone and find ways to network with each other.
The following link provides an insight into what
life is like for schizophrenic. It describes the life a young girl named Jani
who was diagnosed with full blown schizophrenia by the age of six along with
other children that currently live with this diagnosis.
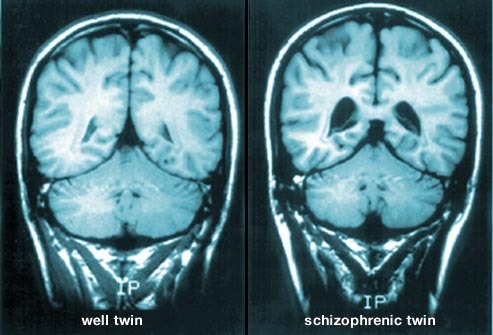
The
following images compare the brains of normal people to people who suffer from
schizophrenia.

What Is Grid-Computing?
Grid-computing is a new computing technology that is now
being used to help find cures for many different diseases, global warming, and
many other types of scientific research. With this technology, any
technological device that uses a computer brain can be voluntarily signed up to
be used to compute different problems. With the amassed computational
power obtained by combining the power of many electronic devices, the
computational power created is greater than the power of a supercomputer.
Basically, a problem is first identified by a scientist/researcher. Once
identified, the work of solving the problem is split up into different pieces
that are all processed at the same time by many different computational devices
during their “idle” time (in the background). By doing so, every possible
way of solving the problem is addressed quickly, reducing the time it takes to
research a problem from years to months. Not only is this a more
efficient way of performing research, but it is also less expensive, allowing
money to be allocated to other things.
What Is Our
Contribution to Schizophrenia?
We will be contributing to the study of Schizophrenia by
taking a part of the Mind Modeling grid by downloading its section in the GPU Grid. Mind Modeling is a nonprofit organization that
is based in based in Dayton, OH at the Wright State University and the
University of Dayton Research Institute. This project not only looks at
Schizophrenia but it also focuses on different cognitive problems in order to
increase the knowledge of cognitive science. It is geared towards understanding
the different cognitive processes that enable human interaction in order to
gain a better insight of the human mind. The section of the GPU Grid from Mind Modeling that we will be contributing to will be assessing the affects of sodium ions have in the binding of anti-psychotic drugs to D2 Dopamine receptors. Understanding these interactions will be very helpful in future drugs created to treat schizophrenia. Our computer will be simulating the effects of sodium ions on dopamine receptors in the brain under psychological ionic strength conditions.
Web Resources:
http://www.nimh.nih.gov/health/topics/schizophrenia/index.shtml?utm_source=publish2&utm_medium=referral&utm_campaign=www.kpbs.orghttp://www.mayoclinic.org/diseases-conditions/schizophrenia/basics/definition/con-20021077
http://www.gpugrid.net/science.php?topic=brain
Subscribe to:
Posts (Atom)